
Fistula Device IFU 2021
Trans-Fistula Insertion
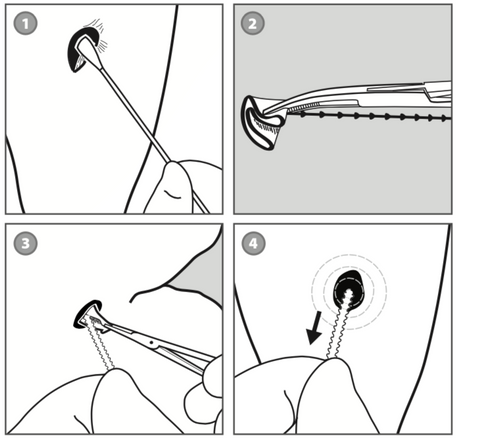
Hand-fold the inner flange of the prosthesis into as small a configuration as possible and grasp it tightly with a hemostat. Also gently grasp the end of the beaded stem, keeping slight tension on the stem for safety (Fig 2).
Gently insert the folded flange through the fistula tract releasing the flange from its folded configuration at the inner aspect of the fistula tract. Withdraw the hemostat while securely holding the end of the beaded stem (Fig 3).
Lightly tug outwardly on the beaded stem to confirm that the flange has deployed and is securely seated against the inner tissue surface (Fig. 4).
Insert the tapered tip on the beaded stem of the prosthesis through the center hole in the outer flange. Move the outer flange down the beaded stem until a “snug” inner-flange-to- outer-flange relationship is achieved that seals sufficiently enough to reduce fistula leakage. Once this flange adjustment is complete, feed the tapered end of the beaded stem through the locking loop, leaving a small amount of slack in the stem to form a curved contour (Fig. 5). Detach the excess stem, leaving 4 to 5 beads beyond the face of the locking loop (Fig. 6). These remaining beads may be needed later for adjustment and/or for prosthesis removal. Test for leakage as described below under “Post-Insertion Inspection”.
Sedated Endoscopic Removal
In the event the physician elects this approach, the inner flange of the fistula prosthesis can be removed in a sedated endoscopic removal procedure. Detach the outer flange from the beaded stem while holding on to the beaded stem. Grasp the stem of the prosthesis with laryngeal forceps or alligator forceps as close as possible to where the beaded stem attaches to the inner flange and withdraw the prosthesis out through the mouth.